
Why we Must Move Away from the Paper Paradigm of the EHR
Opinion – Adam Carewe, MD Co-Chief NerdMD
Treating the Electronic Medical Record (EMR) like a sleek electro-version of the traditional paper chart of yesteryear needs to stop. The mantra of sleuthing through notes to find the information you need should end as well. With modern day software user interface (UI) and user experience (UX) there will be improvements, but that will take time for the vendors to catch up. What can be done today to drive better care for patients?
Two Primary Solutions for Today’s EMR Issues for Improved Patient Care:
- Use Medical, Nursing and Pharmacy Informaticists (like the Chief NerdMDs) to design the flexible parts of the EMR for the best UX/UI and clinical workflow for end users
- Start utilizing tools that break the paradigm of simply documenting notes, by shifting to Problem and Patient Centered Documentation
Historically, EMRs were built to satisfy Meaningful Use requirements (and act as a billing machine/platform) and NOT with UI or UX in mind, so end users and patients continue to suffer. Going back even further to the first iteration of the grandfather of all EMRs, EPIC Systems, the initial iteration was simply a copy of the traditional paper chart. Now you won’t wonder why there is still such a heavy use of “tabs” through the current EMR design!
More recent newcomers to the EHR game (like ePocrates which was acquired by Athenahealth) were actually designed with user experience in mind, and users of this platform experience that advantage. However, for the vast majority of healthcare providers using an EMR, this is not the case (all you EPIC and Cerner users!)
Let’s look a little deeper into the two primary bullet points from above:
- Use Medical, Nursing and Pharmacy Informaticists (like the Chief NerdMDs) to design the flexible parts of the EMR for the best UX/UI and clinical workflow for end users
Health Care team members (including physicians, nurses, pharmacists, and other providers) with strong fundamental knowledge of clinical medicine, but also technically savvy in understanding the current state of their EMR (and most importantly) where the EMR vendor is going in the short and long term future have the clear advantage. Building a robust Clinical Informatics teams consisting of experts in medicine, nursing, and pharmacy is paramount to this success. Having this team in place allows workflows to be mapped to current EMR capabilities, rather than taking a proposed clinical workflow, and making it work with the EMR. The latter can get you into trouble, much like trying to fit a square peg into a round hole. It is far superior to start with the round peg and tweek it to fit the ideal workflow and existing framework of the round hole. Also, who knows the patient better than the physicians and teams taking care of the actual patients? Having informatics groups design and consult and build on the system and workflows will lead to more time with a patient, rather than being stuck in an EMR system that was designed as a billing and Meaningful Use engine.
Informatics = Better Patient Care.
“Having this [informatics] team in place allows workflows to be mapped to current EMR capabilities, rather than taking a proposed clinical workflow, and making it work with the EMR. The latter can get you into trouble, much like trying to fit a square peg into a round hole.”
Adam Carewe MD Co-Chief NerdMD
- Start utilizing tools that break the paradigm of simply documenting notes, by shifting to Problem and Patient Centered Documentation
This one’s a bit more difficult because it requires a heavy dose of change management to shift a culture of traditional clinical documentation. In the paper chart days, you had to document your current progress note on a separate piece of paper. You also maintained a paper list of the patient’s current medical problems (Problem List), History, and Medications and Allergies. You then had results, EKGs, imaging reports, etc all filed away behind tabs in chronological order. As you are reading this description of the paper chart, you are probably thinking, this sounds just like the way the EMR is set up…and you are correct for the most part! Sure, the EMR has some filtering to find stuff faster, some trending capabilities for historical results, and even more recently the ability to “Google” the chart for what you are looking for. All of these examples have clear advantages over paper, but there continues to be little innovation into how we document a patient’s chronic/ongoing problems.
“This one’s a bit more difficult because it requires a heavy dose of change management to shift a culture of traditional clinical documentation.”
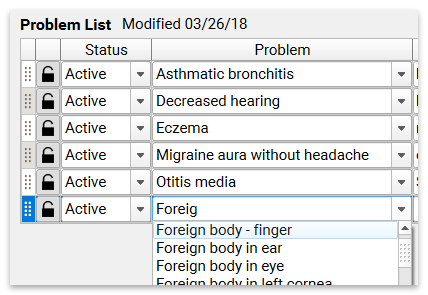
This brings up the paradigm shift to Problem Based Charting, which I feel is critical to changing the way we document and manage a patient with an EMR. Imagine if you opened up a Chart of a new patient to you and all their Acute and Chronic issues are clearly documented along with a brief overview of the issue and well as the most current assessment and plan for each condition, along with automatically linked relevant labs and medications. If you wanted to dive deeper into one condition you could easily open the historical record of the prior assessment and plans to see what has been tried in the past. You could also sort by body system, allowing a specialist to initially only see the grouped relevant conditions to their practice. All of this and more is currently available in most of the leading EMR vendors (specifically EPIC), but getting to this state requires an “all-in” approach to documentation. Every physician and provider needs to document this way for this to be successful. This is difficult, but can be made easier with a robust Clinical Informatics team in place.
Problem Based Charting is the future. Eventually the EMR vendors will get their software to a state that much of this will be automatic, by using natural language processing from voice and text in the medical record to parse out those details and place them into the appropriate place on the Problem List, so the medical record represents a summary of the patient that is easy to review and digest, but also able to dive deeper into those conditions that are pertinent at the time.
We are NOT even close to that state yet. However, starting the shift in your organization to this approach of Problem Based Charting, and utilizing the current tools available, and having informatics teams build new documentation tools to pull this Problem Based/Patient Centric info into traditional progress notes (to satisfy billing and coders) will allow for a seamless transition to when this becomes more automatic in the future with software innovations and advancements.
Physician Informaticists Join the Conversation on LinkedIn and Facebook
Keep the conversation going by replying to this post or joining the NerdMD LinkedIn or Facebook Groups


